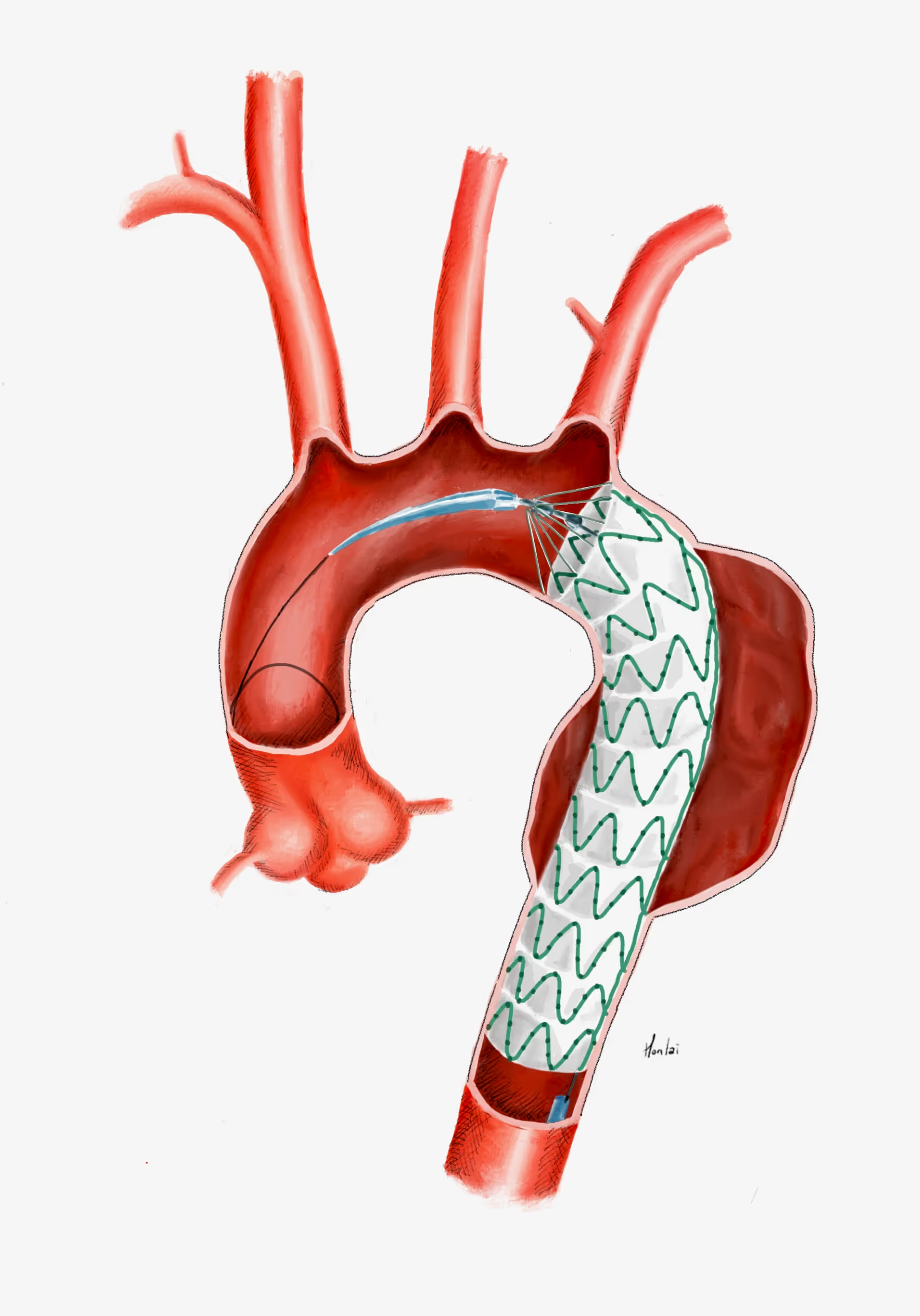
A thoracic aneurysm withat least 20mm of non-aneurysmal aorta between the left subclavian artery and the aneurysm AND at least 20mm of non-aneurysmal aorta between the aneurysm and the celiac trunk can usually be treated endovascularly using a standard off-the-shelf stent graft system. However, some additional anatomical conditions must be met for a successful TEVAR. These include but are not limited to a cylindrical (as opposed to conical) neck; a neck diameter between 20and 42 mm; limited amount of thrombus and calcification in the necks; iliac arteries that allow the introduction of the delivery systems.
Learning targets
.avif)
The Vascular International (VI) School for Vascular Surgery is dedicated to advancing the training and education of vascular surgical techniques through the use of lifelike models. With patient safety as the top priority, VI continuously strives to enhance vascular surgery training, ensuring the highest standards of safe and effective open and endovascular patient care.
About Us